
The Size Thresholds, the Bosniak System, and When Your Doctor Should Be Concerned
| Quick Answer
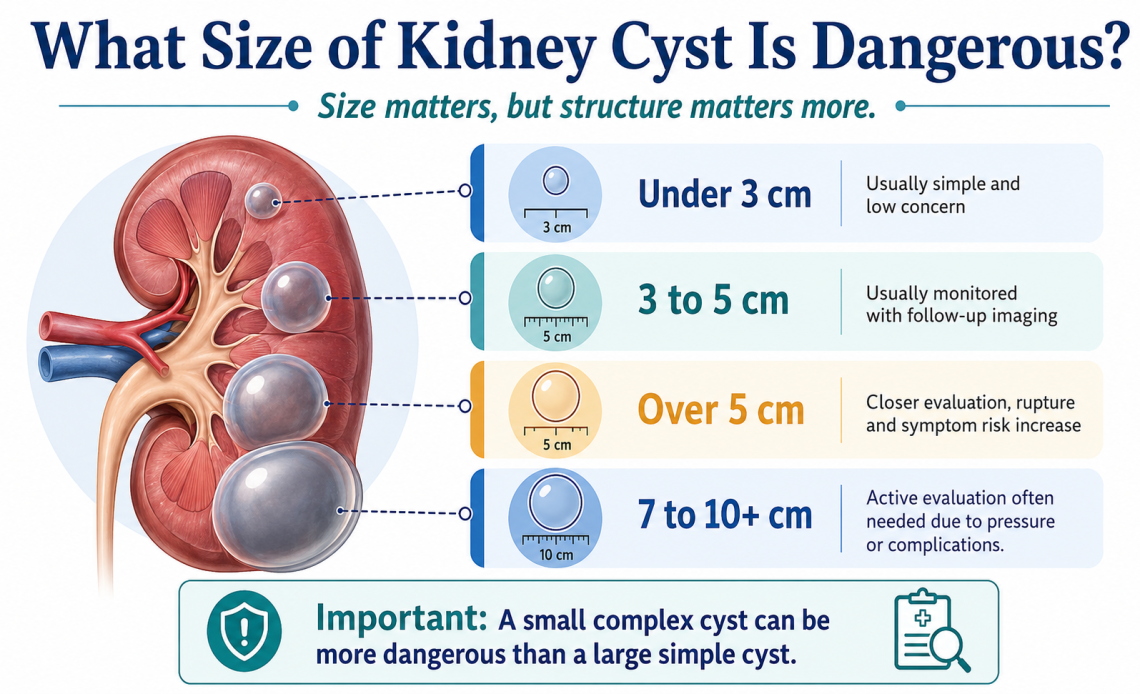
There is no single size that automatically makes a kidney cyst dangerous — structure matters as much as size. That said, most clinicians use these practical thresholds: cysts under 3 cm (30 mm) in a simple, fluid-filled form are almost always benign and need no treatment. Cysts between 3–5 cm warrant monitoring. Cysts over 5 cm (50 mm) carry an 8-fold increased rupture risk and typically require closer evaluation. Very large cysts exceeding 7–10 cm may need intervention. Crucially, a small complex cyst with thick walls or internal debris can carry up to 40% malignancy risk regardless of size — structure and the Bosniak classification system ultimately determine danger more reliably than a number alone. |
Kidney Cyst Danger — Everything at a Glance
| Factor | Details |
| What a Kidney Cyst Is | A fluid-filled sac that develops in or on the kidney — usually discovered incidentally during imaging for another reason |
| How Common | More than 50% of adults over age 50 have at least one kidney cyst; the vast majority are benign |
| Simple vs. Complex | Simple = fluid only, smooth thin walls = almost always harmless. Complex = thick walls, internal divisions (septae), calcium deposits, or solid areas = warrants further evaluation |
| Under 3 cm | Rarely requires treatment; less than 1% complication risk over five years if simple |
| 3–5 cm | Monitoring recommended; treatment if symptomatic or showing complex features |
| Over 5 cm (50 mm) | 8-fold increased rupture risk; typically requires closer evaluation and possible intervention |
| Over 7–10 cm | May require active intervention regardless of structure due to mass effect and complication risk |
| Bosniak I / II | Benign — no treatment needed; routine follow-up only |
| Bosniak IIF | Follow-up required; up to 12% malignancy risk |
| Bosniak III | 50–80% malignancy risk — surgical discussion typically indicated |
| Bosniak IV | 90%+ malignancy risk — surgery generally recommended |
| Warning Symptoms | Flank or back pain, blood in urine, fever, new hypertension, feeling of fullness or pressure |
| Emergency Symptoms | Sudden severe flank pain (possible rupture), high fever with chills (possible infection), rapid symptom worsening |
| Key Takeaway | Size guides monitoring; structure (Bosniak category) determines cancer risk. A large simple cyst may be less dangerous than a small complex one. |
You Got Your Scan Results. Now You Are Staring at a Number.
It happens the same way for most people. A scan for back pain, a routine check after another health concern, or a follow-up ultrasound, and buried in the report is a phrase you were not expecting: kidney cyst, 3 centimetres. Or 5 centimetres. Or 47 millimetres.
The number gets circled. Questions start forming. Is this dangerous? Does it need to come out? Should I be worried? What does the size actually mean?
The honest answer from the research is this: size matters, but it is not the whole story. In fact, for kidney cysts, the structure of the cyst, what it looks like on imaging, not just how big it is, often tells you more about risk than the diameter alone. So, What Size of Kidney Cyst Is Dangerous? This guide covers both sides of that picture so you can have an informed conversation with your doctor rather than a frightened one.
What Exactly Is a Kidney Cyst — and Are They Common?
A kidney cyst is a sac filled with fluid that develops in or on the kidney tissue. Most contain a clear, straw-coloured fluid similar in composition to urine. They form from small tubules in the kidney — tiny channels that play a role in filtering blood — that become blocked or dilated over time.
They are extraordinarily common. Research consistently shows that more than half of adults over the age of fifty have at least one kidney cyst. Many people develop them without any symptoms, never find out they have them, and live perfectly normal lives. The cysts are discovered during imaging done for an entirely different reason — which is why kidney cysts are among the most frequently encountered incidental findings in modern medicine.
The vast majority are benign. The challenge is identifying the small minority that are not — and that is where size, structure, and the Bosniak classification system become important.
What Size of Kidney Cyst Is Actually Considered Dangerous?
Here is the direct answer that most people come looking for — with the important caveat that follows it.
| Size | Risk Level | Typical Clinical Response | Key Note |
| Under 1 cm (10 mm) | Very low | Observation only — often not even formally followed up | Almost always incidental and benign; rarely documented as a clinical concern |
| 1–3 cm (10–30 mm) | Low | Routine monitoring in most cases; imaging follow-up may be recommended | Less than 1% complication risk over five years for simple cysts in this range; risk begins rising meaningfully after about 1.5–2 cm |
| 3–5 cm (30–50 mm) | Moderate | Regular imaging follow-up; treatment if symptoms develop or complex features present | Cysts in this range tend to cause pressure symptoms if positioned near the ureter or adjacent structures; monitoring frequency increases |
| Over 5 cm (50 mm) | Higher | Closer evaluation; strong consideration of intervention if symptomatic | Rupture risk increases 8-fold at this threshold; can cause pain, infection, and bleeding requiring emergency care |
| Over 7–10 cm | High | Intervention typically recommended regardless of symptoms | Mass effect on surrounding structures; higher risk of complications; surgery or aspiration more commonly indicated |
| Any size with complex features | Depends on Bosniak category — potentially very high | Further imaging, specialist referral, possible surgery | Complexity — thick walls, septae, calcification, enhancement — overrides size as the primary risk indicator |
The important caveat: these are clinical guideposts, not hard danger lines. A 6 cm simple cyst that is stable, symptom-free, and has been unchanged on three consecutive scans may be managed conservatively. A 2 cm cyst with thick internal walls and enhancing tissue on CT scan may go directly to surgical consultation. Your doctor weighs size alongside structure, symptoms, growth rate, and your overall kidney function.
What Is the Bosniak Classification — and Why Does It Matter More Than Size?
The Bosniak classification system was developed to give doctors a standardised language for describing kidney cysts on imaging. It moves beyond size and looks at what the cyst actually looks like — its walls, internal structure, calcification pattern, and how it behaves with contrast dye on a CT scan.
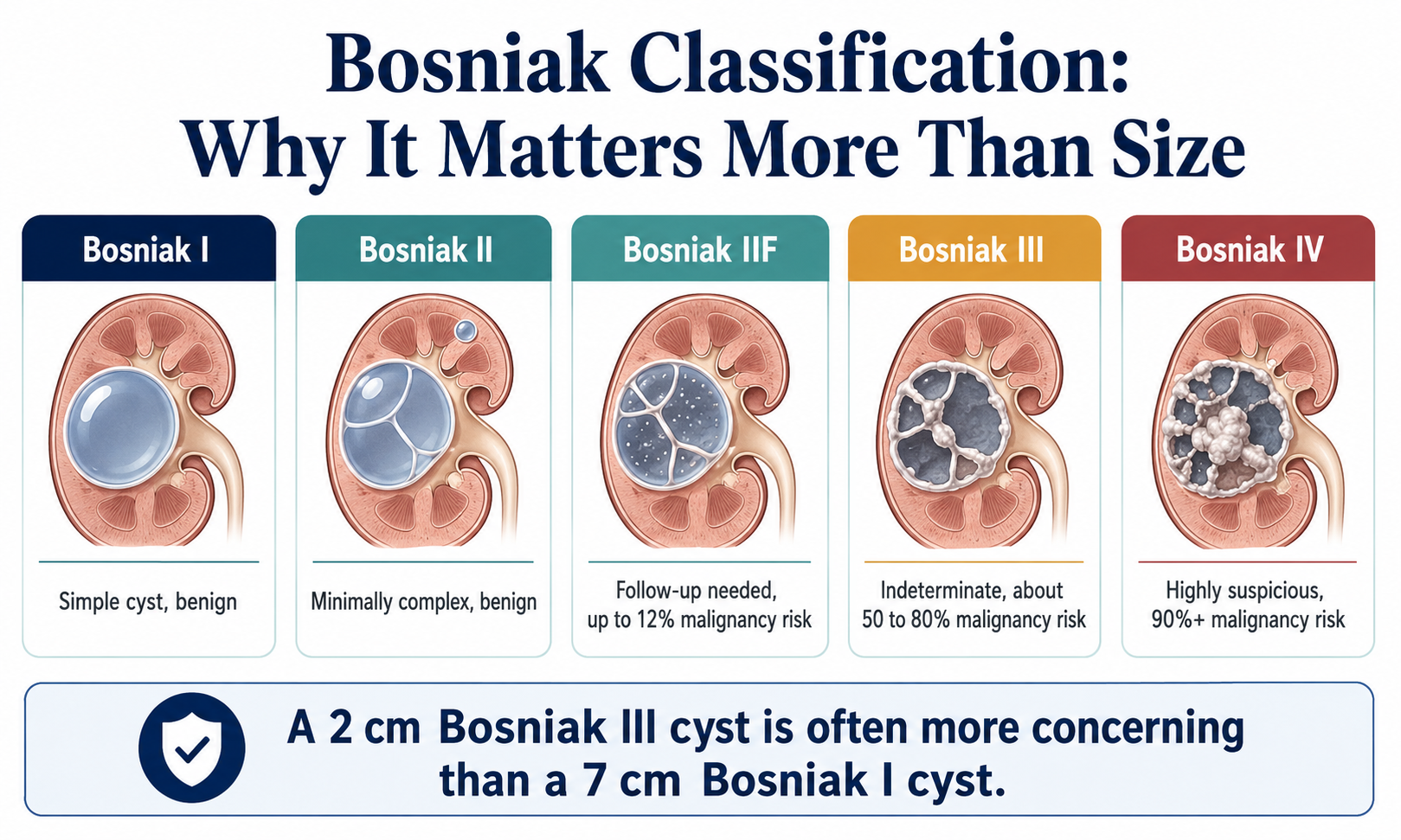
Understanding your Bosniak category is arguably more important than knowing the measurement in centimetres — because a Bosniak I cyst of seven centimetres is almost always less dangerous than a Bosniak III cyst of two centimetres.
| Bosniak Category | What It Looks Like | Cancer Risk | Typical Action |
| Bosniak I | Simple cyst — completely fluid-filled, hairline-thin smooth wall, no septa, no calcification, no enhancement with contrast | Essentially zero | No follow-up needed in most cases — benign by definition |
| Bosniak II | Minimally complex — may have one or two thin septa, fine calcification in the wall or septa, small and well-defined | Essentially zero | No follow-up needed; benign |
| Bosniak IIF | More complex — multiple thin septa, thicker or nodular calcification, no measurable enhancement; larger (over 3 cm) | Up to 12% | Follow-up imaging at 6–12 months; progress to Bosniak III classification if features worsen or growth occurs |
| Bosniak III | Indeterminate — thick, irregular or smooth walls, thick septa, measurable enhancement; cannot exclude malignancy | 50–80% | Surgical consultation typically recommended; partial or full nephrectomy in many cases |
| Bosniak IV | Clearly malignant — all features of Bosniak III plus enhancing soft-tissue components independent of walls or septa | 90% or higher | Surgery generally recommended; urgent specialist referral |
Bosniak III and IV cysts require action regardless of their size. A Bosniak IV cyst of 1.5 cm carries a ninety percent or higher malignancy risk — far more dangerous than a Bosniak I cyst of 10 cm. This is the core point that most people researching kidney cyst size miss entirely.
Simple vs. Complex Cysts — What Is the Difference and Why Does It Change Everything?
| Feature | Simple Cyst | Complex Cyst |
| Contents | Clear fluid only | May contain debris, blood, or protein-rich fluid |
| Wall thickness | Hairline thin, smooth | Thick, irregular, or nodular |
| Internal structure | None — completely hollow | May contain septa (internal divisions), solid areas |
| Calcification | None or fine and peripheral | Thick, irregular, or coarse calcification |
| Enhancement on CT | No enhancement with contrast dye | May show measurable enhancement — key malignancy indicator |
| Bosniak category | I or II | IIF, III, or IV depending on specific features |
| Cancer risk | Essentially zero | 12% to over 90% depending on category |
| Action needed | Routine monitoring or no follow-up | Further imaging, specialist referral, possible surgery |
| Key takeaway | Size is the main variable — most are harmless | Structure overrides size as the primary risk indicator |
When Should Symptoms — Not Just Size — Make You Call Your Doctor?
Many kidney cysts cause no symptoms at all, even when they are large. The presence or absence of symptoms is one of the key factors that pushes a cyst from watchful waiting to active management.
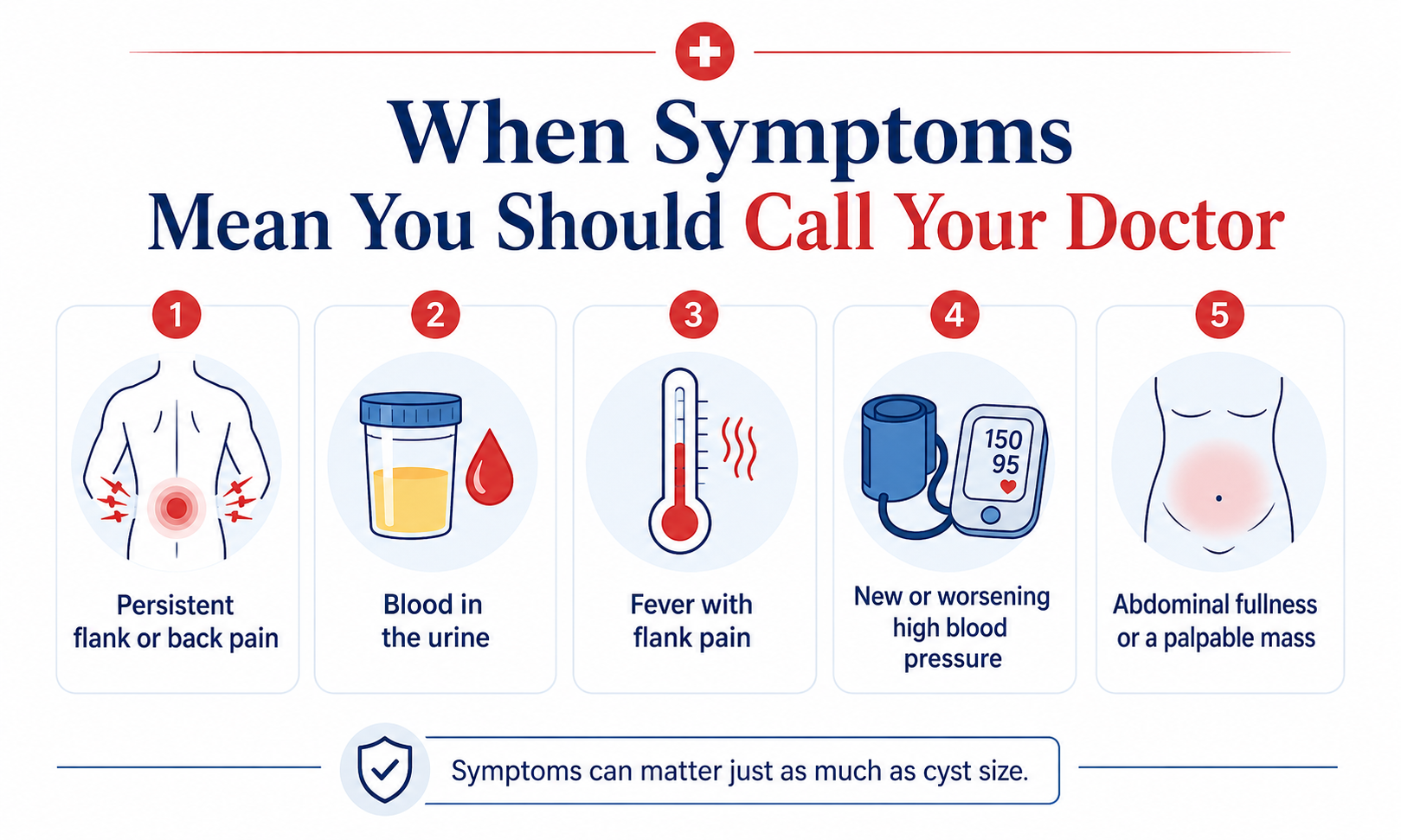
The following symptoms warrant prompt evaluation, regardless of whether you already know your cyst size:
- Persistent flank or back pain. An ache or dull pain on one side of your back or abdomen — particularly if it is new, worsening, or accompanied by other symptoms — can indicate the cyst is pressing on surrounding structures or has developed a complication.
- Blood in the urine (haematuria). Visible or microscopic blood in urine associated with a known kidney cyst can indicate bleeding into the cyst or surrounding tissue and requires prompt evaluation.
- Fever with flank pain. This combination raises concern for an infected cyst — a serious complication that typically requires hospitalisation and antibiotic treatment.
- New or worsening high blood pressure. Large cysts can compress renal blood vessels, activating hormonal pathways that raise blood pressure. New hypertension in someone with a known kidney cyst is a clinically relevant finding.
- Feeling of abdominal fullness or a palpable mass. Very large cysts can cause a sensation of pressure or fullness in the abdomen and may occasionally be felt externally.
| Seek Immediate Medical Attention For:
Sudden, severe flank pain (possible cyst rupture) — Fever above 38.5°C with chills and flank pain (possible infected cyst) — Rapid worsening of any of the above symptoms — Blood in urine accompanied by severe pain. Cyst rupture, though uncommon, can cause significant internal bleeding requiring emergency intervention. |
How Do Doctors Decide Whether to Monitor, Treat, or Remove a Kidney Cyst?
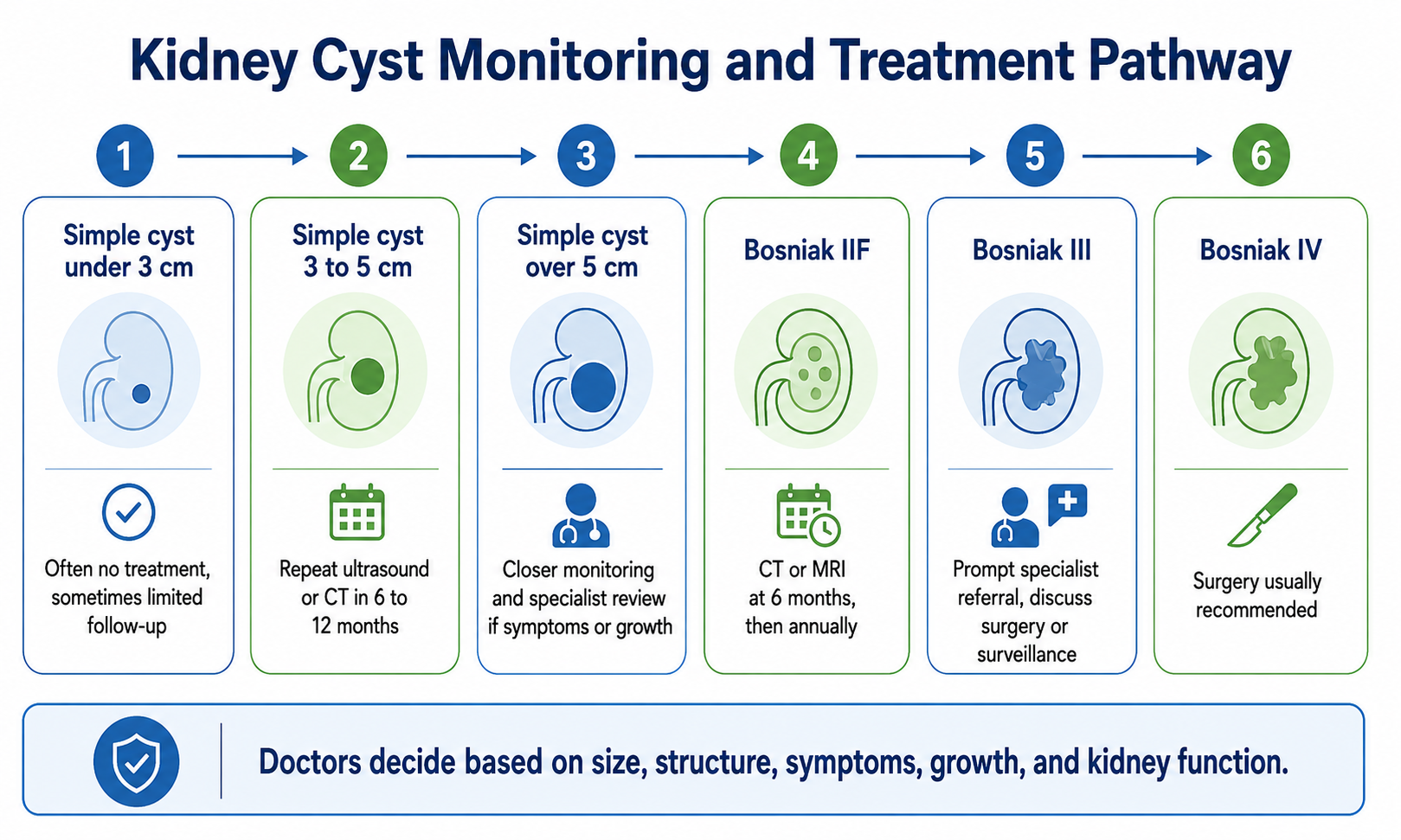
The clinical decision is never based on size alone. Your doctor weighs five factors together to determine the right path forward.
| Factor | What the Doctor Is Assessing | Why It Matters |
| Size | Absolute measurement in centimetres and whether it has grown on serial imaging | Growth rate is often more informative than absolute size — a stable 6 cm cyst may be less concerning than a 3 cm cyst that has doubled in six months |
| Structure (Bosniak category) | CT or MRI appearance — wall thickness, septa, calcification, enhancement | The single most important factor for cancer risk; overrides size in determining urgency |
| Symptoms | Pain, haematuria, hypertension, infection, urinary obstruction | Symptomatic cysts of any size warrant treatment consideration; asymptomatic large cysts may be observed |
| Kidney function | eGFR (estimated glomerular filtration rate) and split kidney function on imaging | Large cysts can reduce functional kidney volume; declining eGFR in a patient with multiple or large cysts changes the management priority |
| Patient factors | Age, overall health, comorbidities, patient preference | An 80-year-old with a Bosniak IIF cyst may be managed very differently from a 45-year-old with the same finding — risk tolerance for surgery differs significantly |
What Happens After Diagnosis? — The Monitoring and Treatment Pathway
Understanding the typical pathway removes a lot of the fear around receiving a kidney cyst diagnosis. Here is how most cases move through the system:
Simple cyst, under 3 cm, no symptoms: Often discharged with no formal follow-up, or a single repeat scan in one to two years to confirm stability. No treatment required.
Simple cyst, 3–5 cm, no symptoms: Repeat ultrasound or CT in six to twelve months to confirm stability. If stable, monitoring interval extended. If growing, further imaging and specialist referral.
Simple cyst, over 5 cm, no symptoms: More frequent monitoring — typically every six months. Specialist referral if symptoms develop or growth is documented. Aspiration or surgery considered if cyst causes complications.
Bosniak IIF cyst, any size: Follow-up CT or MRI at six months, then annually. If features worsen or growth is documented, reclassification and surgical consultation.
Bosniak III cyst, any size: Specialist referral promptly. Discussion of surgical options — typically partial or radical nephrectomy. Active surveillance in selected low-risk patients.
Bosniak IV cyst, any size: Surgery generally recommended. Treated as presumed malignancy until proven otherwise.
What Do People Get Wrong About Kidney Cyst Size and Danger?
- “A bigger cyst is always more dangerous.” Not true. A ten-centimetre simple Bosniak I cyst is far less dangerous than a two-centimetre Bosniak III cyst with enhancing tissue. Size without structural context is an incomplete picture. The Bosniak category is the primary cancer risk indicator, not the diameter.
- “If it is not painful, it is not serious.” Many dangerous kidney cysts cause no pain at all — particularly early-stage malignant cysts. Pain is one of several factors your doctor considers, but its absence does not rule out a significant finding.
- “All complex cysts are cancer.” Bosniak IIF cysts carry up to twelve percent malignancy risk — which means eighty-eight percent are not cancer. Even Bosniak III cysts have a significant proportion that turn out to be benign after surgery. Complex does not automatically mean malignant.
- “Kidney cysts shrink on their own.” Simple kidney cysts do not typically resolve on their own. They may remain stable for years or grow slowly over time. They do not spontaneously disappear. Rapid shrinkage of a cyst should itself be reported to a doctor, as it can occasionally indicate a ruptured or drained cyst.
- “Once a kidney cyst is removed, the problem is solved.” Kidney cysts can recur. People who develop one simple cyst are statistically more likely to develop additional cysts over time. Regular monitoring continues after treatment to catch recurrence or new lesions early.
Which Treatment Option Is Right — and What Are the Trade-offs?
| Treatment Option | Best For | Pros | Cons |
| Watchful Waiting / Monitoring | Simple cysts (Bosniak I–II); asymptomatic cysts under 5 cm; stable cysts on serial imaging | No procedure required; no recovery time; appropriate for the majority of kidney cysts | Requires ongoing imaging; some patient anxiety with repeated scans; growth can occur between monitoring intervals |
| Aspiration (Needle Drainage) | Symptomatic simple cysts causing pain or pressure; cysts compressing adjacent structures | Minimally invasive; no general anaesthesia required; effective short-term relief | High recurrence rate — fluid refills in most cases within months to years; not curative; does not address complex cyst features |
| Aspiration with Sclerotherapy | Symptomatic simple cysts where aspiration alone has failed or is unlikely to be durable | Better long-term results than aspiration alone; still minimally invasive | Recurrence rate lower but not zero; sclerosing agent causes some discomfort; specialist procedure |
| Laparoscopic Cyst Decortication (Surgical Unroofing) | Large symptomatic simple cysts recurrent after aspiration; complex cysts requiring tissue sampling | Low recurrence rate; definitive treatment for symptomatic cysts; allows tissue biopsy | Requires general anaesthesia; surgical recovery; small procedural risks |
| Partial or Radical Nephrectomy | Bosniak III–IV cysts with significant malignancy risk; confirmed renal cell carcinoma | Definitive treatment; removes cancer if present; potentially curative | Major surgery; significant recovery; partial loss of kidney function (partial) or complete loss of one kidney (radical) |
What People Keep Asking About Kidney Cyst Size — Answered Directly
Is a 4 cm kidney cyst dangerous? A simple 4 cm cyst with no symptoms and no complex features is typically managed with monitoring rather than treatment. It sits at the threshold where most clinicians recommend imaging follow-up every six to twelve months. If it causes pain, grows rapidly, or shows complex features on imaging, the management becomes more active.
Is a 5 cm kidney cyst serious? A 5 cm simple cyst is at the threshold where rupture risk increases significantly. It requires closer evaluation and regular monitoring. Most clinicians will order more frequent imaging and discuss intervention if symptoms develop. A 5 cm complex cyst with suspicious features is treated very differently — it may go directly to surgical consultation.
Can a kidney cyst become cancerous? Simple Bosniak I and II cysts essentially never become cancerous. The risk of malignancy rises with cyst complexity — Bosniak IIF carries up to 12% risk, Bosniak III 50–80%, and Bosniak IV 90% or higher. The structure of the cyst, not its size, is what determines cancer risk.
What is the difference between a kidney cyst and kidney cancer? Most kidney cancers (renal cell carcinoma) are solid tumours, not cysts. However, some kidney cancers present as complex cystic lesions — which is why the Bosniak classification was developed. A simple fluid-filled cyst with thin walls and no enhancement is almost certainly benign. A cyst with solid enhancing components has a high probability of malignancy and requires further investigation.
Do kidney cysts affect kidney function? Simple single cysts rarely affect kidney function. Research shows that risk to kidney function begins rising meaningfully once cysts exceed about 1.5 to 2 cm and increases further with multiple cysts. Very large cysts can compress functioning kidney tissue and reduce the GFR (filtration rate) of the affected kidney. Regular eGFR monitoring is recommended for patients with larger or multiple cysts.
How often should a kidney cyst be monitored with imaging? Monitoring frequency depends on Bosniak category and size. Bosniak I and II cysts often need no formal follow-up. Bosniak IIF typically requires imaging at six months, then annually. Simple cysts over 3 cm are usually monitored every six to twelve months initially, with intervals extended if stable. Your doctor will tailor the frequency to your specific case.
What Most Articles on This Topic Get Wrong — and What the Research Actually Shows
The majority of content about kidney cyst danger focuses on a single size number — usually five centimetres — as if crossing that threshold automatically means danger. What the actual clinical evidence shows is considerably more nuanced.
Research from large cohort studies has found that risk to kidney function begins rising meaningfully at around 1.5 to 2 cm, not at five centimetres. Having multiple cysts compounds this risk independently of any individual cyst size. A patient with four separate two-centimetre cysts may warrant more attention than a patient with one stable five-centimetre simple cyst.
The other thing most guides miss is the Bosniak IIF category — the follow-up group. Patients in this category have cysts that do not yet meet the threshold for surgical recommendation but carry up to twelve percent malignancy risk. Many patients are told “it is complex but not cancer” and interpret this as no serious risk. The twelve percent figure means that roughly one in eight of these cysts is malignant. Consistent follow-up is not optional for this group — it is the safety net.
Most people do not realise that the debate around kidney cyst management has shifted in the last five years. There is increasing interest in active surveillance even for low-risk Bosniak III cysts in older patients with significant surgical risk — rather than defaulting to immediate surgery for everyone in that category. The decision is becoming more individualised, which is why the conversation with your specialist matters as much as the scan result.
The Bottom Line — What to Take Into Your Next Appointment
There is no single dangerous size. The honest clinical answer is that a 3 cm simple cyst is almost certainly harmless, a 5 cm cyst warrants monitoring, cysts over 7–10 cm require active evaluation, and the complexity of the cyst — not the size — determines cancer risk.
If you have received a kidney cyst diagnosis, the most useful thing you can do before your next appointment is find out your Bosniak category. Ask your doctor specifically: what does this cyst look like on imaging, not just how big is it? That question will get you further than any number alone.
What to avoid: making treatment decisions based on size alone, dismissing a smaller cyst with complex features as low-risk because it is small, and ignoring symptoms — particularly flank pain, blood in urine, or new high blood pressure — while waiting for a scheduled monitoring appointment.
Most kidney cysts are benign and require nothing more than periodic scans. For the minority that are not, early identification through the Bosniak system gives the best possible chance of effective treatment.
The Decision Framework — What Should You Do Based on Your Situation?
| Your Situation | Most Likely Category | Recommended First Step |
| Simple cyst under 3 cm, no symptoms, discovered incidentally | Bosniak I or II | Ask your doctor if monitoring is even needed — many in this group require no formal follow-up |
| Simple cyst 3–5 cm, no symptoms | Bosniak I–IIF | Confirm structure with CT if not already done; establish a monitoring schedule — typically six to twelve months |
| Simple cyst over 5 cm, no symptoms | Bosniak I–IIF | Specialist referral; more frequent monitoring; discuss intervention options if the cyst grows or causes symptoms |
| Cyst of any size with thick walls, septa, or internal debris | Bosniak IIF–III | CT or MRI with contrast for full characterisation; specialist referral; discuss Bosniak category specifically |
| Cyst with solid enhancing components on imaging | Bosniak III–IV | Urgent specialist referral; surgical consultation; treat as presumed malignancy until fully evaluated |
| Any cyst with pain, blood in urine, or fever | Symptomatic — any category | Prompt medical evaluation — do not wait for a scheduled monitoring appointment |
| Any cyst with sudden severe pain | Possible rupture | Emergency department immediately |
Myth vs. Reality — The Quick Reference
| Myth | Reality |
| Bigger always means more dangerous | A large simple cyst is often less dangerous than a small complex one — structure determines cancer risk more than size |
| No symptoms means no problem | Malignant cysts frequently cause no symptoms in early stages — regular monitoring is essential regardless of how you feel |
| All complex cysts are cancerous | Bosniak IIF carries up to 12% malignancy risk — 88% are not cancer; even Bosniak III has a significant proportion that are benign |
| Kidney cysts eventually go away on their own | Simple cysts do not self-resolve — they typically remain stable or grow slowly over years |
| A single size number tells you everything | Bosniak category, symptoms, growth rate, number of cysts, and kidney function together determine the full picture — size alone is incomplete |